What is wrong with the model which prompted lockdowns? An interview with Andrea Molle
As the spread of COVID19 progressed rapidly in Europe at the beginning of 2020, the pandemic predictive model devised by the Imperial College in London featured prominently in public policies and debates. Its extremely worrying statistics prompted lockdowns.
Now, it’s under intense scrutiny.
Researcher Andrea Molle (Chapman University, California), who covered several aspects of COVID19 in a series of previous articles, explains what is wrong with it and the way it entered public debate.
What do you make of the criticism surrounding the model and its author, Professor Neil Ferguson?
I would not go as far as Elon Musk and call him a fake. That was wrong and unwarranted. He is undoubtedly an impressive and reputable scholar. But Prof. Ferguson also has a record of excessively pessimistic predictions and mortality overestimations. For example, look at his work on the 2001 foot and mouth epidemic up to his recent incorrect prediction of 2009 swine flu mortality. They were both calling for draconian measures but ended up in nothing.
How do you evaluate the model itself?
First, I would like to start by saying that I believe that models should not be looked at as infallible predictions but as tools to explore probabilistic scenarios. If we look at a model as a prophecy, like we have done so far with COVID-19, then we end up fulfilling it hoping to avoid an even more catastrophic outcome. The issue I have with this model, in particular, is not with the model per se. But, the ease with it was assumed as the “golden standard” to inform global suppression, and mitigation strategies, is frankly unacceptable.
Why?
In my opinion, it was a decision based more on the reputation of the Imperial College than its applicability as a policy tool, which is quite frankly very limited.
Why do you believe so?
Mainly because the model is too simplistic to inform policies. I do like an elegant model, but the complexities of this pandemic call for more sophisticated approaches. Without getting too technical, Ferguson’s model is based on an assumption of an R0, the linear reproduction number, which is assumed to be randomly distributed in the population. This assumption, otherwise legitimate, ignores something we need to know in estimating a contagion: how social and cultural factors determine the spread of contagion in modern societies, making a huge difference. Also, the model is, quite frankly, unsound to inform policies for it cannot be empirically tested.
The model became the golden standard because it was a convenient choice for politicians looking for a magic bullet approach that minimized their responsibilities and the potential fallout.
Can you elaborate on that?
Let me give you an example. Imagine a scenario where I am telling you, “don’t go outside, or you are going to die because the rain is going to kill you.” Faced with such an extreme outcome, you rationally decide to stay in and eventually survive. Can I use this as proof that I was right and the rain kills? Not at all. Would 10,000 people not going out and not getting killed good enough to prove my statement? Again, it is not enough. It is not a matter of numbers. I have to prove that, first, people by sending people outside to die; second, that they die because of the rain and, lastly, that there is nobody (of course, allowing a certain level of tolerance) that goes outside, get wet, and survives. How can I test all of that without risking people’s lives? And how about testing the use of a raincoat, or an umbrella, with a subset of the population? Going back to our suppression and mitigation strategies, informed by Fergusson’s model, no one took the risk of doing nothing and saw what would happen: if the model were empirically sound. And even if some countries, like Sweden or Japan, did something close to that, supporters of the dominant narrative do not consider it enough of evidence that the model was wrong. And rightfully so.
On the other hand, because in many countries we have fewer numbers of what the models predicted in its worst-case scenario, that is automatically taken as evidence that the model is 100% correct. All of it without excluding alternative explanations, which is a must in addressing causal hypothesis. A typical way of reasoning of what we call an “unfalsifiable” theory, in other words, an unscientific one. I don’t believe this was Ferguson’s intention, but it is how the model entered the political debate.
The model ignores something we need to know in estimating a contagion: how social and cultural factors determine the spread of contagion in modern societies, making a huge difference.
Is the model wrong?
I am not saying it was “wrong.” A model is not wrong or right; it is consistent with its assumptions and the data used to fit it. I am simply saying that there is no way to tell if its predictions were valid. The model is designed, or at least presented, in a way that does not allow itself to be tested. Of course, I am not implying that social distancing is not essential and should not be carried out. It does matter, and we know it from the epidemiological literature. But there are different ways to apply it, and we should have also considered other models, and opinions, before committing ourselves to such an extreme strategy as an indiscriminate lockdown under any circumstances.
So why did it become the golden standard?
Because its outcomes, and the inferred policies, are simple to understand and, politically speaking, safe to implement. It was a convenient choice for politicians looking for a magic bullet approach that minimized their responsibilities and the potential fallout.
The problem is that there is no magic bullet, and decisions should be tailored to each country’s specific context. Even more so, areas within countries should have different strategies based, among other things, on their population and network structures. An increasing number of scientific publications, based on real data, is showing that some are might need a full lockdown, whereas others might do better with targeted closures. Also, there are now better mathematical and computational models that account for these social, economic, and cultural differences. Still, they are not as immediate as Ferguson’s to understand. And not as simple to turn into policies to fight COVID-19 without taking a huge political risk. Unfortunately, adopting Ferguson’s model without asking for a second opinion or double-checking, it might have been a wrong choice.
The consequence of adopting an extreme, blanket, strategy is that there is now a mounting pressure to abandon any form of social distancing completely.
Are you referring to the accusation that the model was badly coded? What if the model is, like it is suggested now, faulty and full of mistakes?
I was not directly referring to that. If those accusations, however, are proven right, it will turn up to be a huge scandal, which will potentially cause massive lawsuits. More importantly, it will start an unprecedented wave of mistrust in, if not open hostility towards, science and politics. After all it could be considered partially responsible for the dare social and economic consequences of the pandemic.
In what sense then. And what conclusions can we draw?
The consequence of adopting an extreme, blanket, strategy is that there is now a mounting pressure, fueled by the long-term unsustainability of the current approach, to abandon any form of social distancing completely. Politicians will eventually succumb to the pressure, and this would potentially lead to a dire scenario. Ironically, that might provide the data we need to validate or disprove, Ferguson’s model.
Comorbidity Factors (such as heart disease and diabetes) Influence COVID-19 Mortality More Than Age (Chapman University)
by Steven Gjerstad and Andrea Molle – Chapman University, USA
last update 2020.03.30
“It is an extremely important finding, not only because it allows for better decisions in the triage phase. But also because in the following phases, starting from the so-called phase 2 up to the production and distribution of a vaccine, it will be essential to make decisions aimed at protecting those who are the most at risk of serious consequences. Moreover, before the vaccine is distributed, individuals with hypertension, diabetes, heart disease, if not already developed immunity, will necessarily have to be closely monitored. Not only as they are at higher risk, but above all because if the disease is reactivating, we will see it in those with comorbidities, since healthy individuals tend to be asymptomatic and therefore could spread the virus silently.”
THE RESEARCH
The global reaction to the COVID-19 epidemic has rested on a critical assumption, that all persons over the age of 60 face an unacceptable risk of death if they are infected with the virus. Recent evidence from a detailed analysis of individual Chinese, American, and Italian patient data clearly indicates that this assumption is incorrect. Our research indicates that only 0.8% of all coronavirus-related deaths in Italy involved otherwise healthy individuals. The remaining 99.2% of deaths involved individuals who had at least one, and often at least 3 other illness factors. There are significant public policy implications to our quarantine and triage strategies.
Mortality from COVID-19 increases substantially with comorbidity factors, such as heart disease, hypertension, diabetes, stroke, and liver disease. After we control for the high incidence of comorbidity factors among the elderly, we find that mortality from coVid-19 does not vary much with age.
The coronavirus epidemic in Italy has strained hospital resources, including ICU beds and ventilators for those experiencing acute respiratory failure. Studies of COVID-19 in China [1], Italy [2], and the United States [3] show that fatality rates increase rapidly with age, especially beyond age 60. The same studies and others also show that fatalities increase substantially with comorbidity factors, such as heart disease, hypertension, diabetes, stroke, and liver disease [1, 4]. These morbidity factors are known to increase rapidly with age [5, 6, 7]. This paper demonstrates that once we control for comorbidity factors, age has a minor effect on COVID-19 mortality. Among the elderly the higher incidence of heart disease, diabetes, hypertension, and other comorbidity factors lead to their increased mortality form COVID-19. The distinction is an important one for the critical triage decisions that are required now. If it is the comorbidity factors that lead to death with COVID-19 patients and not age, then triage will be more effective if healthy elderly people are provided with treatment, since their chances of survival are good.
We examine 73,780 cases of COVID-19 and 6,801 deaths from COVID-19 in Italy through March 26, 2020. Based on estimates of the prevalence of comorbidity factors in Italy by age group and on the frequency of COVID-19 cases and mortality rates for age groups, we estimate the percentage of patients with and without morbidity factor that would be expected to die, first assuming that those with and without comorbidity factors are equally likely to die. Subsequently, we use a maximum likelihood estimate to get mortality probabilities for people in each age group, with and without comorbidity conditions. COVID-19 patients with comorbidity conditions are 10.5 times as likely to die than those without a comorbidity condition. For example, an Italian COVID-19 patient between 70 and 79 years old with no comorbidity factor has about a 1.6% chance of death, whereas a 70 to 79 year-old patient with a comorbidity condition has a 21.4% chance of death.
Triage decisions based on patient age do not account for the large differences between the prognosis for patients with and without morbidity factors. As medical resources become strained during the epidemic, it will be important to take account of the probabilities of survival for patients with different medical histories.
Analysis
Table 1 in [4] shows that 50.7% of the fatal cases of COVID-19 in Italy through March 26 had 3 or more of the comorbidity factors. Another 25.9% had 2 of these factors, and 21.3% had one factor. Only 2.1% had no factor. This last statistic is important. If age alone were an independent factor that leads to high mortality, then – we will demonstrate in this paper – there would be many more deaths among those who are elderly but otherwise healthy. In other words, the 2.1% frequency of no comorbidity factors would be much higher.
Tabella 1 in [8] shows that 19.2% of 73,780 COVID-19 cases in Italy through 4 p.m. on 26 March were among people age 70 to 79. From Tavola 7 in [7], we can infer that close to 25% of those people have none of the comorbidity conditions. We take death rates for the age groups from Tabella 1 in [8]. We consider the hypothesis that healthy people in each age group are as likely to die as those with 1 or more comorbidity condition. This hypothesis will lead us to the conclusion that there should be approximately 10.5 times as many people with no comorbidity factors as the number that are shown in Table 1 in [4].
People between 70 and 79 comprise 19.2% of the cases, and 25% of those have no comorbidity condition, so healthy people 70 – 79 years old are 4.8% of the cases. If healthy people between the ages of 70 and 79 are as susceptible to death from COVID-19 as those in their age group who have comorbidity conditions, then their death rate should be 16.9%, like their age group. If they were dying at the same rate as their age group, the fraction of all cases who would be people between 70 and 79 and have no comorbidity factor would be 0.048 x 0.1569 = 0.0081. Now we repeat this analysis for the remaining age groups and fill out Table 1.
Table 1: Column E shows the percentage of the 73,780 total cases that would be healthy people (i.e., no comorbidity factor) in their age group and would die from COVID-19.
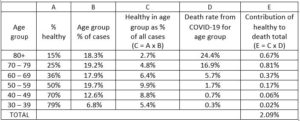
The total number of deaths that we would expect for people with no comorbidity factor would be this expected death frequency times the number of cases, which is 0.0209 x 73,780 = 1,542.
Table 2: Column E shows the percentage of the 73,780 cases in each age group that would die who have one or more comorbidity factor.
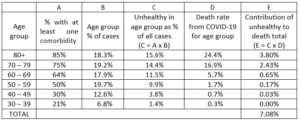
We now carry out a similar calculation in Table 2, but we consider here those people who have one or more comorbidity factor. This calculation shows that 7.08% of the total cases should be people with one or more comorbidity factor who died. That would result in 0.0708 x 73,780 = 5,223 deaths. As a check, total predicted deaths are 6,765. The total number of deaths from Tabella 1 in [8] where we get our total number of cases and our lethality factors for age groups (Column D) is 6,801.3
Our hypothesis that healthy people in each age group have the same probability of dying from COVID-19 leads us to the conclusion that of our estimated 6,765 deceased, 1,542 or 22.8% should have no comorbidity factor. Yet Tabella 1 in [4] shows that only 2.11% had no comorbidity factor. Consequently, the hypothesis that the probability of dying is the same for all people in an age group regardless of their comorbidity factors leads to the conclusion that there would be about 10.8 times as many deaths among those with no comorbidity factor than what we see in the sample of deceased persons in Tabella 1 in [4].
This analysis can be augmented by assuming different probabilities of mortality for those with and without comorbidity factors. If we multiply every element in Column D in Table 1 by 0.0925 we would get 143 deaths among those with no comorbidity factor. If we multiple every element in Column D, Table 2 by 1.2677 we would get 6,622 deaths among those with one or more comorbidity factor. We would then have 143/6,765 = 2.11% of the deceased having no comorbidity factor, as in Tabella 1 in [4]. The probabilities of death are then those in Table 3.
Table 3: These mortality probabilities produce fatalities in each age group that match total fatalities and match the frequency of comorbidities found in Tabella 1 in [4].

From this we conclude that age is most likely only a moderate factor leading to COVID-19 mortality. Of course, healthy elderly patients are not dying in large numbers from COVID-19, so triage decisions that ignore the elderly healthy are not likely to lead to large numbers of deaths within this group. These patients are likely to recover, but they are likely to recover more quickly and with less physical damage if they are provided treatment. They also are unlikely to require critical care for much longer than a healthy young person, since like the healthy young, they are recovering. For these reasons, we believe that triage decisions should be made without regard to a patient’s age.
About the authors
Steven Gjerstad, PhD, Economic Science Institute, Chapman University, 1 University Drive, Orange, California, 92866 USA, E-mail: gjerstad@chapman.edu; Tel: 714-628-7282
Andrea Molle, PhD, Institute for the Study of Religion, Economics and Society, Chapman University, Orange, California, 92866 USA
References
[1] Wu, Zunyou and Jennifer M. McGoogan, “Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China,” Journal of the American Medical Association, Feb. 24, 2020.
[2] Livingston, Edward and Karen Bucher, “Coronavirus Disease 2019 (COVID-19) in Italy,” Journal of the American Medical Association, March 17, 2020.
[3] “Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020.” Centers for Disease Control, Morbidity and Mortality Weekly Report (MMWR), 18 March 2020. DOI: http://dx.doi.org/10.15585/mmwr.mm6912e2
[4] “Report sulle caratteristiche dei pazienti deceduti positivi a COVID-19 in Italia,” Instituto Superiore di Sanita, 20 Marzo 2020.
[5] “Age-adjusted percentages of selected circulatory diseases among adults,” Centers for Disease Control, Summary Health Statistics: National Health Interview Survey, 2018. https://ftp.cdc.gov/pub/Health_Statistics/NCHS/NHIS/SHS/2018_SHS_Table_A-1.pdf
[6] “Diabetes prevalence and glycemic control among adults,” Centers for Disease Control, 2018. https://www.cdc.gov/nchs/data/hus/2015/040.pdf
[7] “Patologie croniche in costante aumento in Italia con incremento della spesa sanitaria. La cronicità non colpisce tutti allo stesso modo: si confermano le diseguaglianze di genere, territoriali, culturali e socio economiche,” Istituto di Sanità Pubblica, Roma, 15 febbraio 2019. https://www.osservatoriosullasalute.it/wp-content/uploads/2019/02/Focus-1-Osservasalute-La- cronicità-in-Italia-feb-2019.pdf
[8] “Epidemia COVID-19 Aggiornamento nazionale,” Istituto Superiore di Sanità (ISS), Roma, 26 Marzo 2020.


 per la sicurezza nazionale e la cooperazione regionale")




















